When we are checking babies to make sure their blood glucose is acceptable, we are doing so to prevent brain injury. However, since we only measure blood glucose and not the amount of ketone bodies, pyruvate or lactate, we get a number. A number that tells us glucose levels but doesn’t measure alternative sources of energy: a random number flying through the air.
So, let’s say have new term baby with a measured glucose of 28.
Does that baby have symptoms? Kids without symptoms are doing something right. We do not need to intervene because our exam told us the baby looked good. The number did not add to our management and therefore we did not need it. That glucose of 28 may mean nothing if the baby makes up for it with creation of alternative fuels (which they do normally). Kids with no symptoms from their low blood sugar (however we define it) do not need to be treated. Our next step is to do what we should be doing already: skin-to-skin snuggling, feeding within an hour after birth, and frequent breastfeeding with rooming-in.
When we treat an asymptomatic child with a "low" blood sugar (again, however it is defined) with something other than breastmilk, the production of alternative fuels gets messed up. The baby needed a low blood glucose to start the pathways that create alternative fuel production. When we give formula or glucose water, we are giving glucose, and those other pathways that created ketone bodies, pyruvate and lactate as compensation for the low blood sugar are now not needed. Those other newborn pathways may be delayed in working or just stop. Because we messed with normal physiology, and may have interrupted alternate fuel production, the babies may need continued supplementation to maintain normal blood glucose.
The production of alternative fuels does not just work to meet the energy needs of the brain. Ketone bodies are also used in brain myelination (nerve growth) and the creation of lung surfactant (lung function). That means that the normal dip in blood glucose, which creates other fuels, leads to brain energy, nerve growth and lung development. We want that to occur without interruption. We should not supplement a normal, term, asymptomatic baby with low blood glucose.
A baby with a low blood sugar and symptoms, well, that’s a problem. Symptomatic blood sugar can show up as irritability, seizures, lethargy, turning blue, coma, not being able to maintain your temperature, irregular breathing, among other evil things. Now look at that list and see if we want to chalk any or one of those symptoms up to just a low blood sugar. That baby could be sick. Really sick. Like "take them to the ICU sick."
What’s up with that baby that they didn’t compensate for their low glucose with those ketone bodies? What went wrong? Maybe the baby is premature, or late-preterm and can’t create ketone bodies or alternative body fuel because their liver is not mature enough. Maybe the baby is simply cold and should be snuggling on mom’s chest. Or maybe that baby has overwhelming infection, congenital heart disease, lung disease, liver disease or is otherwise really sick. Kids with low blood sugar and symptoms can have awful neurological problems. We need to investigate, with urgency, the reason that the baby could not make a normal metabolic transition.
SO…
Low blood sugar with no symptoms. Not an issue.
Breastmilk meets the nutritional requirements of healthy, term infants and those same healthy term exclusively breastfed infants do not develop low blood sugar because they are not eating. Healthy term infants do not need to have their blood sugar screened.
Low blood sugar with symptoms: Big problem.
These children have some reason they can’t make up for low blood sugar with other fuels. They may be, among other things, premature, small for gestational age, an infant of a diabetic mother (especially if the diabetes was poorly controlled), be sick, or be withdrawing from a substance mom was taking. Those kids should be screened because then, the number means something.
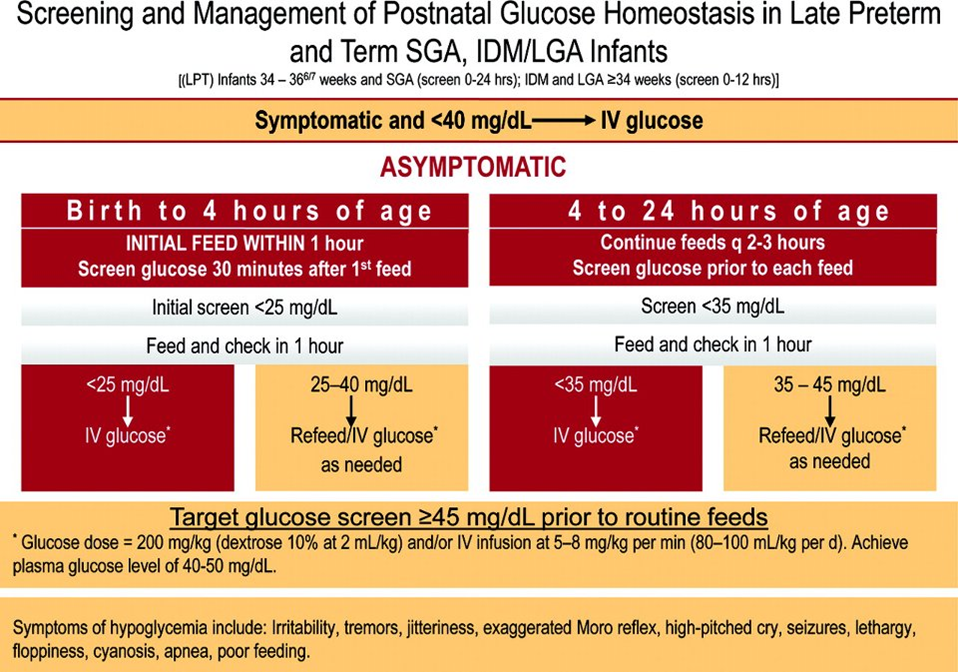
The American Academy of Pediatrics addressed this issue of newborn hypoglycemia in 2011
with a clinical report which acknowledges many of the things that we don't know about low blood sugar such as what glucose concentration in the newborn is considered normal and how long the glucose needs to be low in order to cause neurologic injury. In the clinical report, the authors created an algorithm to help target at-risk children. The kids they recommend we screen are only in three categories: small for gestational age babies; babies of diabetic mothers (and controversially) large for gestational age infants; late preterm babies, defined as those born at 34- 36 6/7 weeks. No other baby needs to be screened. Here it is:
Jenny Thomas, MD, MPH, IBCLC, FAAP, FABM